





Study design and participants
This study used a matched historical controlled study design, aiming to compare the changes in orthopedic surgical care quality indicators before and after the implementation of the standardized surgical CP. The study population consisted of patients undergoing orthopedic surgery during the study period and their registered nurses responsible for perioperative care. Inclusion criteria: all patients undergoing elective orthopedic surgery during the study period, and the surgical nurses involved in their perioperative care were included in the study. Exclusion criteria: patients who underwent emergency surgery, had a history of repeat surgery, or had serious comorbidities that could interfere with postoperative outcomes were excluded. Specifically, patients with a preoperative diagnosis of infection or severe sepsis, as well as patients with grade IV surgical incisions, were excluded from the analysis, based on the National Academy of Sciences’ stratified wound classification system [10, 11].
Study setting
The study was conducted in a large general hospital in China with more than 1,900 beds covering more than 52 medical specialties and care provided by more than 2,500 professionals. The department of surgery is equipped with 20 ORs and a team of more than 70 specialist nurses supporting a wide range of surgical procedures, including orthopedics, urology, general surgery, and cardiac surgery. The department provides surgical services to over 30,000 patients annually. The data collection period was from July 1, 2019, to June 30, 2024, a time span that allowed us to comprehensively assess the long-term impact of CPs on the quality and efficiency of orthopedic surgical care. The study was approved by the Institutional Ethics Review Board (IRB) under number 2024-22. All individuals who participated in the study and agreed to the release of their identifying information or images signed a written informed consent form, and the research process strictly adhered to the ethical principles of the Declaration of Helsinki.
Intervention
The control group adhered to a traditional, non-standardized CP with personalized care activities based on the individual patient’s needs, while the intervention group implemented a standardized CP to improve the quality of care through a systematic approach and teamwork [12].
Staffing, training, and management of CP
OR nurses assume a variety of roles, ranging from administrative oversight to professional team leadership and direct patient care. Nurses at all levels are assigned specific responsibilities guided by a patient-centered care philosophy. Intraoperative CPs were guided by experienced team leaders and supported by members with at least one year of experience. A “standardized training” model has been implemented, which focuses on progressive professional development with a curriculum designed by the OR education secretary and tailored to different levels of expertise. This training system consists of three years of standardized training and two years of specialized training in the OR, covering basic system protocols, standardized procedures, crisis management, and specialized surgical procedures [12].
Implementation of Surgical CP
The surgical CP has been carefully designed to enhance the efficiency of orthopedic surgery and improve patient prognosis. The pathway is divided into preoperative, intraoperative, and postoperative phases, each with standardized processes and individualized interventions to ensure high-quality care and patient safety [13, 14] (see Table 1).
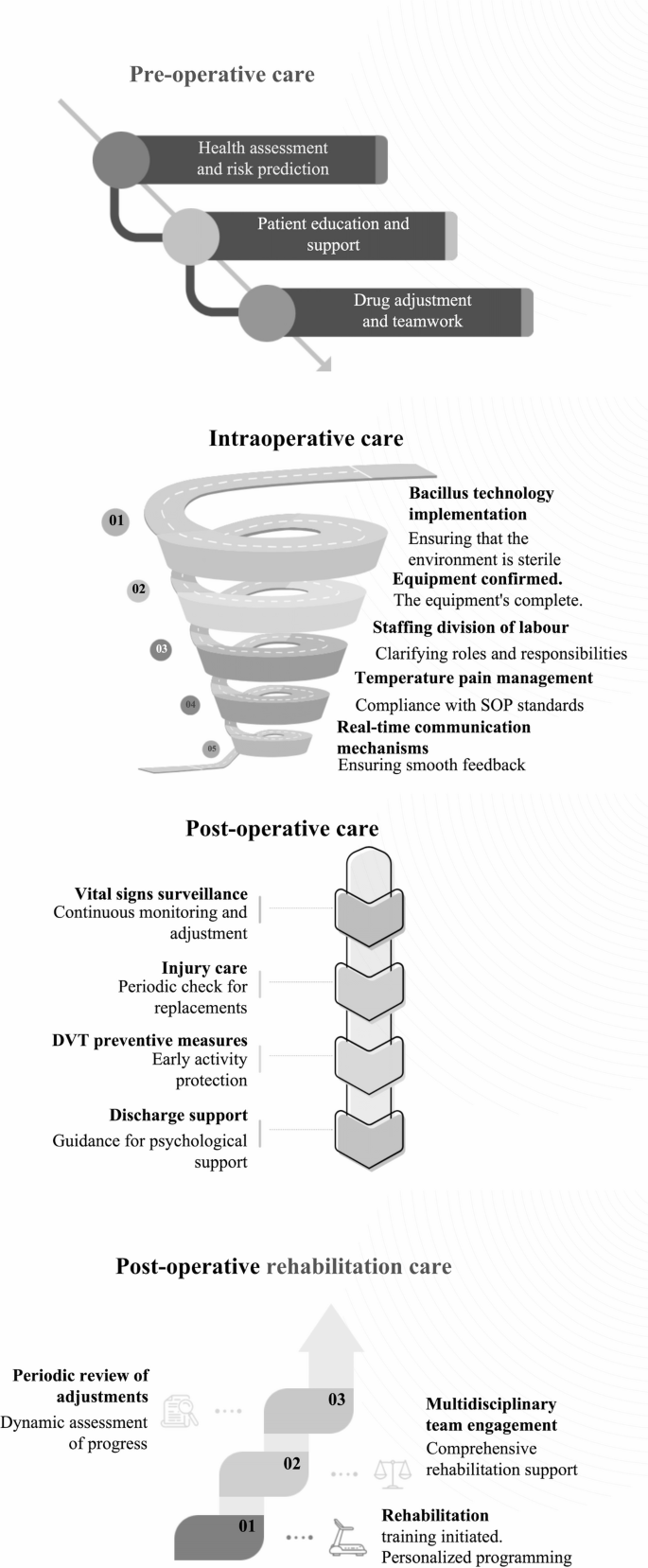
Flow chart of the surgical care pathway
Preoperative care
Comprehensive assessment and individualized risk prediction
The preoperative phase of care begins with the implementation of a comprehensive patient assessment process. A healthcare team of physicians and nurses is responsible for performing a physical examination, medical history review, and laboratory tests to assess whether the patient has indications for surgery and to identify potential risk factors. This assessment is usually completed within 1–2 weeks prior to surgery. Subsequently, standardized risk assessment tools (e.g., ASA score, Charlson Comorbidity Index [15]) are used to predict the probability of SSIs and other complications, and individualized prevention strategies are developed accordingly.
Patient education and health behavior intervention
Next was the patient education session, in which nurses and health education specialists explained the surgical procedure in detail to patients and their families, including the purpose of the surgery, expected outcomes, postoperative recovery, and provided information on pain management, wound care, and rehabilitation training. The dietitian provides personalized dietary advice based on the patient’s nutritional status and prescribes nutritional supplements when necessary to ensure that the patient is in the best condition for the surgery. At the same time, patients are instructed in self-management, such as dietary adjustments and lifestyle changes. For smokers or alcohol drinkers, psychologists or nurses will provide support services for smoking and alcohol cessation 4–6 weeks before surgery.
Medication adjustment and preoperative preparation standards
Medication adjustments are an important part of preoperative care. The physician adjusts the medications being used, especially anticoagulants, one week prior to surgery based on the patient’s condition and surgical needs to minimize surgical risk. In addition, preoperative fasting and glycemic control criteria are confirmed: patients are allowed to drink water two hours before induction of anesthesia, but no solid food should be consumed for six hours prior to surgery to reduce insulin resistance and catabolic state. Routine sedation is not recommended for anxiety relief; acetaminophen, nonsteroidal anti-inflammatory drugs (NSAIDs), and gabapentin are recommended as part of multimodal analgesia. Anemia should also be assessed and corrected preoperatively, and iron or erythropoietin therapy should be given if necessary to reduce the need for allogeneic blood transfusions.
Multidisciplinary collaboration and family support
To ensure consistency and completeness of the treatment plan, a multidisciplinary team meeting is organized in which surgeons, anesthesiologists, nurses, and other relevant personnel discuss each patient’s treatment plan and clarify the preparations. Social workers or nurses invited patients’ families to participate in the meeting to help them understand the surgical process and key points of post-operative care, and to enhance the role of the family support system. Through these meticulous pre-operative preparation measures, not only is the safety and success rate of the surgery improved, but also a better perioperative experience is provided to the patients.
Intraoperative care
Aseptic operation and equipment preparation
During the surgical execution phase, OR nurses strictly enforce aseptic techniques and thoroughly clean the surgical area using highly effective antiseptics, a process that lasts from 30 min before the start of the surgery until the end of the procedure. The technical support staff, in collaboration with the OR nurses, conducts a thorough inspection of all required instruments and equipment to ensure that they are in good working order and develops a contingency plan to deal with any unforeseen circumstances that may occur. The OR supervisor is responsible for rationalizing the division of labor among the staff to ensure that each step of the process is handled by a dedicated person, usually one hour before the start of the procedure.
Clarification of team roles and standardized procedures
Thirty minutes before the start of surgery, the surgical team members clarify their roles and responsibilities to ensure that each member is clear about his or her own tasks, such as monitoring vital signs and recording the procedure. Surgical procedures are customized based on the individual case, the surgeon’s experience, and the hospital’s facilities. During surgery, an effective communication mechanism is established to facilitate information sharing and rapid problem-solving among team members, and this real-time feedback mechanism is important for improving the safety and efficiency of the surgery. All team members strictly adhere to pre-established standard operating procedures (SOPs) to ensure that every step is of the highest standard.
Temperature management and analgesic fluid control
Anesthesiologists work closely with nurses to maintain normal levels of patient body temperature and take measures to prevent hypothermia, such as intravenous fluid warming and preheating equipment. At the same time, multimodal analgesic strategies, including epidural morphine, local block, or long-acting infiltrating anesthetics, were implemented to optimize postoperative pain management. Strict fluid management is performed during surgery, with precise control of the volume and rate of infusion and the use of balanced intravenous fluids to maintain isotonicity and prevent complications due to fluid imbalance. Nursing care at this stage is a key component in ensuring smooth surgery and patient safety.
Postoperative medical care
Vital signs monitoring and analgesia management
During the postoperative care phase, the nurse is responsible for continuously monitoring the patient’s key vital signs, such as blood pressure, heart rate, respiratory rate, and oxygen saturation, to ensure that the patient remains stable during the postoperative recovery period. This process begins immediately after the patient’s surgery and continues until discharge. Doctors and nurses adjust medication dosages according to a pre-established multimodal analgesia program to ensure patient comfort and reduce pain and discomfort after surgery.
Complication prevention and incision care
Nurses regularly inspected surgical incisions to prevent infection and changed dressings in a timely manner. A series of measures were taken to prevent common complications: routine use of urinary catheters was avoided, and if needed, they should be removed within a few hours after surgery; routine use of wound drainage was not recommended, especially after short-segment lumbar fusion, to promote early recovery. Encourage patients to be active early and use compression stockings or anticoagulants to reduce the risk of deep vein thrombosis (DVT). Assess the risk of postoperative nausea and vomiting (PONV), use a variety of medications for prophylaxis, and instruct patients on dietary modifications to reduce symptoms. Strictly enforce hand hygiene practices and limit the number of visitors to minimize the chance of cross-infection.
Discharge guidance and psychological support
In addition, social workers and nurses explain to patients and their families what to expect after discharge, including guidance on medication, arrangements for follow-up consultation, and handling of emergencies. Psychological counseling or support group services are also provided to help patients cope with anxiety and stress after surgery. The goals of nursing care at this stage are to promote patients’ recovery, prevent complications, and lay the foundation for subsequent rehabilitative care.
Post-operative rehabilitation care
Early feeding and individualized recovery plan
Post-operative rehabilitation care emphasizes early feeding to speed up the recovery process. Rehabilitation specialists and doctors develop individualized rehabilitation training plans based on the patient’s specific condition and recovery and set short- and long-term rehabilitation goals, such as regaining normal mobility and returning to work. These programs are usually initiated in the 1 st week after the patient is discharged from the hospital.
Exercise training and nutritional support
Physical therapists instruct patients in appropriate exercise training, gradually increasing the intensity, and teach home exercise methods to promote the recovery of daily mobility and physical function. To address the risk of thromboembolism, early mobility out of bed and the use of mechanical prophylaxis were encouraged, and the use of anticoagulants was considered on an individualized basis. Dietitians and health advisors provide individualized dietary advice based on the patient’s physical condition to promote wound healing and overall health.
Mental health and regular follow-up
Continue to emphasize the importance of smoking cessation and alcohol restriction to avoid compromising the recovery process. Psychologists and social workers provide psychological counseling or support group services to help patients cope with post-surgery anxiety and stress, and arrange counseling sessions to help patients develop a positive mindset. Doctors and nurses arrange regular reviews for patients, usually every 2–4 weeks, to assess the progress of recovery and adjust the treatment plan to prevent other complications. Rehabilitation outcomes are assessed using standardized tools and documented. Postoperative rehabilitation care is a critical phase in achieving functional recovery and improving quality of life.
The standardized nursing process is based on the standardized nursing care path formulated by the department. The responsible nurse cares for patients according to the care path table, which consists of a reference time for CP, an actual execution time for CP, the content of CP, an evaluation of effect, and the signature of the person who executed CP. Nurses provide continuous, dynamic, targeted, and standardized health education to patients from preoperative to postoperative stages based on the CP path. The implemented educational content is marked with a blue pen, while unimplemented content is marked with a red pen. The reason why the unimplemented content was not carried out must be recorded in the nursing record by the duty nurse [12].
Outcome
The primary outcome metrics focused on the incidence of SSIs during hospitalization, the type of pathogen, and its incidence. Postoperative SSIs, as defined by the Centers for Disease Control and Prevention, involve infections of the skin, subcutaneous tissues, deep soft tissues, or any anatomical site within 30 days after surgery that are diagnosed as SSIs by the surgeon or attending physician and are included in the study period to ensure that the surveillance methodology remains consistent across the two study periods. Secondary outcome indicators covered surgical turnover time, patient satisfaction scores with nurses and physicians, and other indicators sensitive to quality of care. Surgical turnover was defined as the time interval between the end of one surgery and the start of the next, usually including the time required to clean the OR, prepare equipment, and rearrange. A positive event was defined as a turnover time of more than 30 min between surgical procedures [16]. Patient satisfaction scores were collected by means of questionnaires, and patient satisfaction ratings of surgical and related services were usually quantified using a Likert scale (e.g., 1–5), which included, but were not limited to, the attitude of healthcare professionals, surgical outcomes, hospitalization environment, pain management, and transparency of information [17].
Data collection
Patient information and care data, including the type of procedure, duration, SSI events, patient outcomes, and caregiver feedback, are carefully collected through electronic medical record systems and OR records.
Validity and reliability
In this study, we used validation tools with good reliability to improve the validity and reliability of the data [16]. We have extensive experience in care management, and quality indicators were available throughout the data collection period. Consistency was maintained using quality indicators and procedures prior to the study design plan, including procedure-related complications, procedure-related quality indicators, and patient satisfaction. The validity and reliability of the data collection instruments were ensured by validating the accuracy of data entry and using standardized assessment tools and scales. All data were scrutinized, and data entry was performed twice to eliminate input errors. Confounders were controlled for using PSM methods to ensure baseline balance between CP and non-CP periods.
Sample size calculation
The sample size was calculated to be 3,836 patients (1,918 in each group) using G*Power ver. 3.1.9.4 Software. Assuming a baseline SSI rate of 2.6%, with an expected reduction to 1.6% post-CP implementation, a two-sided test was used with an alpha level of 0.05 and a desired power (1 – β) of at least 80% [18].
Statistical analysis
Patients were categorized according to the care management they received during the non-CP and CP periods. Categorical variables were presented as numbers and percentages, whereas continuous variables were described in detail by mean (standard deviation) or median (interquartile range). To compare SSI rates and baseline characteristics between the CP and non-CP groups, standardized mean differences (SMDs) were used. In this study, we used a logistic regression model to estimate propensity scores and a nearest-neighbor matching strategy (minimum caliper value of 0.1) for matching. The multivariate model included baseline characteristics such as age, gender, comorbidities, and type of surgery. Initial screening identified significantly relevant variables by univariate analysis (P < 0.2), followed by stepwise regression to identify key predictor variables and to consider significant interaction effects. Hypothesis testing included checking for linear relationships between continuous variables and logit-transformed dependent variables, independence of observations, multicollinearity (Variance inflation factor (VIF) > 10 indicates a serious problem), and outliers or high-leverage points in the residual distribution. The overall model fit was verified using the Hosmer-Lemeshow goodness-of-fit test, and VIF values were calculated for each variable to remove excessive values or transformed variables. For missing data, a full case analysis was first performed, and then the Multivariate Imputation by Chained Equations (MICE) algorithm was used to generate multiple filler datasets and merge the results through the multiple filler method [19, 20]. To further validate the effect of CP, we calculated the ratio of patients’ ratios and their 95% confidence intervals (CIs) before and after pairing by multivariate logistic regression analysis. The comparisons of secondary outcome indicators were analyzed using the Fisher exact test or chi-square test for count data, and the Mann-Whitney U test or t-test for numerical variables, as appropriate. All statistical analyses were done through SPSS 26 software to ensure robust and reliable results.
link
More Stories
Median Arcuate Ligament Syndrome | Orlando surgeon explains signs, symptoms and treatment
Gyder Surgical announces first commercial surgical cases in the United States performed by Dr. Paul M. Lombardi, M.D., at the Tri-County Orthopedics’ Joint Replacement Institute outpatient center
Bunion Surgery Market Get Facts About Business Strategies 2026 to 2031: Medi-tech Insights